 INTRODUCTION
INTRODUCTION
The following information is a guide to your upcoming surgery. It describes what is likely to happen at the time of surgery. This is a guide only and there may be some individual variations, depending on your individual circumstances and Dr Lawrie will discuss these with you. Please become familiar with this guide and discuss any aspects that you wish to with Dr Lawrie, the anaesthetist and/or the nursing staff. You will be admitted to the ward either the morning of surgery or the night before, depending on the time of day of your surgery. A typical hospital stay is 5-7 days. You will need to travel home in an ambulance on the day of your discharge to protect your new hip joint.
BEFORE SURGERY
You should stop taking anti-inflammatory drugs at least five days prior to surgery as they can increase the chance of bleeding (e.g. Voltaren, Naprosyn, Nurofen, Brufen, Feldene, Naprosyn and Indocid. Celebrex, Vioxx and Mobic are not a problem). It is extremely important that you have no cuts, scratches or sores on your lower limb at the time of your surgery as this can increase the chances of infection. If you do have any cuts, scratches or sores then your surgery will be postponed until these are well and truly healed. On the day of your surgery a nurse will inspect your leg for any lesions.
The nurse will then use clippers to remove any long hair from the hip and dress the hip with an antiseptic solution. Dr Lawrie will also inspect the leg and mark the appropriate leg to be operated on with an indelible marking pen. You should stop smoking prior to your surgery as smoking increases the risks associated with an anaesthetic and the risk of blood clots (DVT) following surgery
ADMISSION
You should not eat or drink 6 hours prior to surgery. You should bring with you:
- Personal effects (nightgown or pyjamas, slippers, dressing gown, toiletries)
- Any medication you are taking
- All relevant x-rays, scans and reports
- Medicare and private health fund membership cards
- This paperwork
Prior to going to the operating room, the ward staff will direct you to
- Have a shower with an antiseptic soap
- Be dressed in a theatre gown and disposable underwear
- Have the limb inspected and dressed with an antiseptic solution and sterile drape
If you wish Dr Lawrie to speak to a family member after the operation please notify the nursing staff with contact details.
THE PROCEDURE
You will be taken into the operating room on a trolley by the nursing staff
The operation will take about 90-120 minutes, but you may spend up to two and a half to three hours in the theatre complex by the time you wait in the pre-operative area, are prepared from your anaesthetic and then woken up in the recovery area.
THE ANAESTHETIC
You will meet the anaesthetist prior to your admission when he will discuss with you the different anaesthetic options. The type of anaesthetic you have will be tailored to your needs, taking into account any medical condition that you may have. You may be given a general anaesthetic (where you are completely asleep) or a regional anaesthetic such as an epidural or spinal anaesthetic where the nerves to the limb are numbed from a needle placed in your back.
THE SURGERY
- You will be placed on the operating table lying on your side.
- Your position on the operating table will be held by a number of bolsters to maintain your position.
- You will be covered in sterile drapes so that only the operation site is exposed.
- Dr Lawrie will check your x-rays and use those to ensure that your new hip is placed in exactly the right position and at the right angle for your hip. Any deformities due to your hip condition can often be corrected by your new hip.
- An incision will be made over the hip joint which will best address the pathology in your hip. The typical incision is about 10cm long, but it may be greater if more access is needed due to individual circumstances. Great care is taken to ensure that the major nerves and vessels about the hip joint are protected. The soft tissue envelope about the hip is carefully retracted exposing the capsule of the hip joint.
- The capsule is then entered; exposing the hip joint itself and an instrument is used at this point to mark your leg lengths so that, at the end of the procedure, we can be sure the leg lengths are satisfactory.

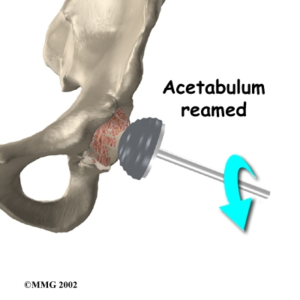
- The hip joint is then dislocated and the ball at the end of the femur is removed. The socket is then assessed and the position of the new socket is determined by consulting the x-rays.
- The socket is reshaped with a special tool on the end of a drill which prepares the socket to a hemispherical shape. Any large bone spurs are removed and any bone cysts seen on your x-ray are plugged with bone from the ball of the femur. A dummy socket is placed to make sure the position is correct.
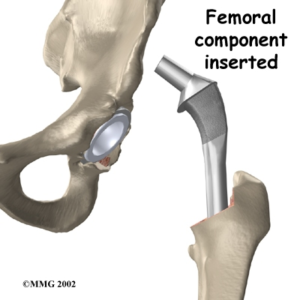
- The femur is then prepared to accept the femoral component. A hole down the centre of the shaft of the femur is prepared which mirrors the shape of the femoral component. A dummy femoral component is then placed into the hole and a ball is placed on the end of it.
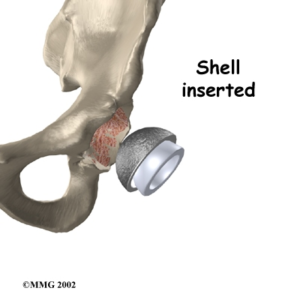
 The dummy hip is then reduced or brought together and the final position of the components is then decided upon. This takes into account the stability of the hip joint (of most importance) the range of motion and the leg lengths. Occasionally the leg lengths of the components and subsequently the patient’s legs need to be adjusted so as to maintain the stability of the joint and not allow the joint to dislocate. This is a very important concept and one that Dr Lawrie will spend some time explaining to you. Once we are happy with the position of the dummy components, the real components will be put into place. Both the socket and the femoral stem can then be put in place, with or without cement.The decision as to which method of fixation to use will depend upon the size, shape and quality of the bone in your hip and the type of pathology in your hip (e.g. osteoarthritis vs. rheumatoid arthritis vs. fracture). Dr Lawrie will discuss this with you prior to your surgery. If bone cement is to be used, its role is to act as a grout to get into all the small spaces within the bone itself. It is not an adhesive and it does not glue the components to the bone. It acts to transmit forces from the components to the bone and load the bone evenly. If cement is not used then the components themselves are fixed to the bone via the surface texture which encourages bone to grow onto the component.These components are typically made of titanium which encourages bone growth. The components are initially stable due to the precise nature of how the bone is prepared to fit the components; they get a mechanical interlock initially. Over time the bone grows onto the implant to give a biological stability.
The dummy hip is then reduced or brought together and the final position of the components is then decided upon. This takes into account the stability of the hip joint (of most importance) the range of motion and the leg lengths. Occasionally the leg lengths of the components and subsequently the patient’s legs need to be adjusted so as to maintain the stability of the joint and not allow the joint to dislocate. This is a very important concept and one that Dr Lawrie will spend some time explaining to you. Once we are happy with the position of the dummy components, the real components will be put into place. Both the socket and the femoral stem can then be put in place, with or without cement.The decision as to which method of fixation to use will depend upon the size, shape and quality of the bone in your hip and the type of pathology in your hip (e.g. osteoarthritis vs. rheumatoid arthritis vs. fracture). Dr Lawrie will discuss this with you prior to your surgery. If bone cement is to be used, its role is to act as a grout to get into all the small spaces within the bone itself. It is not an adhesive and it does not glue the components to the bone. It acts to transmit forces from the components to the bone and load the bone evenly. If cement is not used then the components themselves are fixed to the bone via the surface texture which encourages bone to grow onto the component.These components are typically made of titanium which encourages bone growth. The components are initially stable due to the precise nature of how the bone is prepared to fit the components; they get a mechanical interlock initially. Over time the bone grows onto the implant to give a biological stability.
- The ball and lining of the socket will then be secured. There are a number of different ball/liner combinations that can be used (this is called the bearing surface). Traditionally a metal ball on a hard plastic liner has been used. This works extremely well in the majority of cases, however in the situation of high loading it may wear more quickly than we would hope and it can lead to early failure of the joint. Therefore, a number of alternative bearings have been developed. These include all metal bearing surfaces, ceramic bearing surfaces, new cross-linked plastic bearings and a new ceramic metal called Oxinium. Each have unique characteristics and are useful in certain situations. Dr Lawrie will discuss with you what bearing surface is appropriate for your situation.
- Once the ball and socket are secured, the capsule can be repaired in such a way that will help with stability of the joint. The different muscle layers are then repaired and the skin is closed with staples; occasionally a drain will be placed in the muscle layers and a sterile dressing is then applied.
- You are rolled onto your back and the anaesthetic will be withdrawn by your anaesthetist. A catheter will be placed into your bladder at the end of the operation to prevent any problems with the bladder post-operatively.
THE RECOVERY
You will then be wheeled into recovery and the nurse will monitor your blood pressure, pulse and breathing as you recover from your anaesthetic. A triangular pillow will be placed between your legs so as to control the position of your hip as the anaesthetic wears off. The nurse will check on the sensation and circulation of your limbs.
AFTER SURGERY
- Dr Lawrie will see you and explain the operative findings to you. A copy of the operative report will be sent to your local doctor.
- On returning to the ward you will have a drip placed into your arm; this will keep you well hydrated until you are eating and drinking normally.
- Your blood level will be checked and you may need a blood transfusion.
- You will have tight stockings around both legs which will help to prevent blood clots; these need to be worn for six weeks following your surgery.
- Your usual medications will be given to you.
- You will be placed on antibiotics through the drip for 24hrs to reduce the risk of infection.
- Aspirin will be added to your medications and you should continue to take this for six weeks from the time of surgery to help prevent clots.
- The triangular pillow will be put between your legs while you are in bed to prevent your hip from being put into a position that may dislocate the hip.
- You will be given morphine type medication for pain relief, which may make you drowsy and nauseated.
- Your anaesthetist will keep a close eye on your pain relief and will endeavour to keep you comfortable. Commonly patients will be given a PCA (Patient Controlled Analgesia) which allows you to control the amount of pain killer that is administered through your drip.
- An x-ray of your hip will be taken following your surgery to check on the position of your components. Your blood levels will be checked the following day.
- A physiotherapist will be in charge of your mobility and will visit you following your surgery
- The most important thing you can do after returning to the ward is to get moving as soon as possible. This will help to prevent clots and to maximise your new hip’s flexibility and minimise muscle weakness post surgery.
- You should start with toe wiggling immediately after surgery and progress to sitting out of bed the day after surgery; then walking with the aid of a frame a day or two following your surgery.
- You will be given a number of hip exercises by the physiotherapist, which will aid in getting back your muscle strength and getting you back on your feet.
- You will be ready to leave when you can walk about 30 metres on your own, get in and out of bed, access the toilet and shower, and get up and down stairs successfully
WHEN YOU GET HOME
The risk of dislocation of your new hip joint is highest in the first three months following surgery. Your new hip will feel very good when you are discharged. Often a patient is not aware of their new hip as the pain relief is so good following hip replacement surgery. However, it is very important that you are aware of the risks to your hip and that you follow your hip precautions as described by the physiotherapist.
FOR THE FIRST THREE MONTHS
- DON’T FLEX YOUR HIP GREATER THAN 90°
- DON’T PIVOT OR TWIST ON THE OPERATED LEG
- DON’T SIT FOR LONG PERIODS OF TIME
- DON’T SIT ON CHAIRS WITHOUT ARMS
- DON’T SIT ON OVERSTUFFED FURNITURE
- DON’T CROSS YOUR KNEES OR ANKLES
- DON’T TURN YOUR KNEES TOGETHER
- DON’T SLEEP ON YOUR SIDE
- DON’T BEND TO PICK ANYTHING UP
- DON’T LIE WITHOUT A PILLOW BETWEEN YOUR LEGS
- DON’T SIT IN THE BATH
Once you have your new hip replacement it is up to you to take care of it. Although the new hip replacement may feel much like a normal hip, it is not. It is much like the bearings in a car and it can wear out if too much force is applied to it.
Avoiding excessive and undue stresses on the new hip will give it the best chance of having a long life. You will have to avoid sports involving running or jumping. However, it is important to stay as healthy as possible. Activities such as walking, swimming, golf, lawn bowls and social tennis (preferably doubles) are all encouraged.
It is very important to treat any infections of other areas aggressively such as the urinary tract or dental infections. Many invasive procedures require antibiotics prior to the procedure. It is always best to warn your doctor beforehand that you have a hip replacement as the consequences of an infected hip replacement can be dire.
Surgery on infected hip replacements is extremely difficult and is not always successful at eradicating the infection. One can be left without a hip joint with a painful hip and the leg may be shorter as a result. There is about a 1% chance per year that you will require a revision hip replacement. A hip revision is much more difficult, they tend to have more complications and they have a less successful outcome than the original surgery.
This is why it is so important to look after your new hip forever more. By looking after your hip, you will be able to substantially improve the longevity of your it and hopefully avoid the need for a hip revision in the future.
COMMONLY ASKED QUESTIONS
What are the risks of surgery?
The risks of Hip Replacement Surgery can be thought of as general risks of the procedure and local risks to the hip and leg
General Risks
- Death is possible from the procedure
- There is the risk of having a problem with the heart such as a heart attack, heart failure or arrhythmia
- There is the risk of having a stroke
These events are very rare
- Clots in the legs may occur with pain and swelling of the legs; rarely parts of the clots can break off and travel to the lungs and this can be fatal. Many steps are taken to avoid this from happening.
- Small areas of the lungs can collapse following surgery which may cause infection in the lungs requiring antibiotics and physiotherapy.
- Bladder and prostate problems can be exacerbated by your surgery, but a catheter is routinely placed in your bladder at the time of surgery to avoid this. This will be removed once you are comfortable and mobile.
- The bowel may become paralysed after surgery. This may result in pain, bloating, nausea and vomiting for a short time.
Local Risks
- Infection after hip replacement can occur at any time. Therefore it is very important to be vigilant to the risk of infection. Infection may result in revision of your hip replacement, or you may even be left without a hip; which can often result in a painful and short limb. Sometimes the infection cannot be eradicated, even with further surgery
- The hip can dislocate and it is most at risk in the first three months after surgery, but there is also a lifelong risk. If the hip dislocates it can often be put back in without surgery. Sometimes a brace will need to be worn for a period of time. If the hip continues to dislocate than surgery may become necessary. Surgery for dislocation is extremely difficult with a relatively low success rate. Once again, this shows how important it is to look after your hip replacement.
- The leg length may be different to the opposite side and this may require treatment. Typically a shoe build up is needed, but sometimes further surgery is required. There are many reasons why the leg lengths may be different following surgery. The goal of the operation is to give a pain-free, mobile hip that does not dislocate, and on occasion the leg lengths may need to be altered to achieve this. When the joint is arthritic, cartilage and bone can be lost from the joint; this shortens the leg. When the new hip is put in place, an attempt is made to restore this bone and cartilage loss, therefore the hip is often longer.
- There may be arthritis of the other hip, which is now shorter due to the same process, and once a new hip is in place this leg will be longer. If the hip was very short pre-operatively it can be too dangerous to lengthen the hip to any great degree, so the leg will still be short following surgery.
- The operated hip often feels long initially, even if it is not. In an arthritic hip the soft tissues about the hip joint are scarred and contracted due to the loss of bone and cartilage and with the inflammation about the joint. When the new hip is in place these tissues are initially stretched out of there contracted state and this can feel to you as if the leg is now longer, even if it is not.
- The nerves about the hip joint can be injured at the time of surgery; this can result in pain or weakness or permanent disability. The most common nerve affected is the nerve which supplies the muscles to the top of the foot; damage here can result in foot drop.
- The new hip joint itself may loosen and/or wear over time. This can result in pain and instability over time. The socket, the liner, the head or the stem may fail individually or in combination, which may require revision surgery in the future. Sometimes it can result in bone loss about the hip joint. This can result in fracture of the socket or thigh bone in future years; but a number of steps are taken to reduce the risks of this. Individual circumstances will dictate what type of hip replacement is used so as to get the best result for you.
- There is a risk that the new hip may fail within the first five years. This will require further surgery
- Occasionally the bone of the socket or femur may break at the time of surgery. This is often recognised at the time and can be corrected during the hip replacement. This may mean that you are not able to walk on the hip for a period of time following the surgery. Rarely you may need further surgery to treat the fracture.
- The wound may not heal properly and can become red, thickened and painful; steps are taken to avoid this.
- Possible bleeding into the wound after surgery can occur. This may become painful and require surgical drainage, or it may become infected and require antibiotics.
- There is a risk that the leg may have to be amputated due to poor blood supply or infection.
- There is an increased risk of complications in obese people of wound infection, heart and lung complications and blood clots.
- There is an increased risk of complications with patients who have diabetes.
- There is an increased risk of complications with smokers.
- There is an increased risk of complications for patients with multiple medical problems.
- There is an increased risk of complications in the very elderly and infirm.
Will my surgery be successful?
Hip Replacement surgery is extremely successful; with a very high chance it will substantially improve or completely relieve your pain. There is about a 1% chance per year that you will require a revision hip replacement. Hip revisions are much more difficult, tend to have more complications and will have a less successful outcome than the original surgery. That is why it is so important to look after your new hip forever more.
When can I drive?
You may drive when you are walking without crutches, when you have good quadriceps function and when you no longer require pain killers which may cause drowsiness. This will be approximately six weeks to three months after your surgery.
Download