Introduction
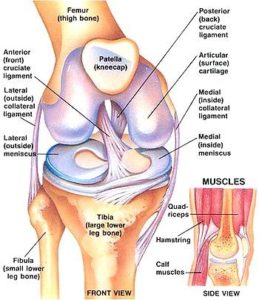
The Anterior Cruciate Ligament (ACL) is a 38mm long band of fibrous tissue that connects the thigh bone (the femur) and the shin bone (the tibia). It runs from front to back through the centre of the joint. It prevents the outer aspect of the tibia moving forward on the femur during twisting type activities. It thereby gives stability to the knee.
It typically is not functioning during normal daily activities such as walking but when the knee comes under load the ACL comes into play. The ACL is essential in controlling forces across the knee in twisting activities such as stepping, pivoting and landing from a height.
 ACL injury
ACL injury
The ACL is commonly injured in sporting situations where a sudden change of direction is associated with a sudden deceleration such as stepping or propping whilst a contact is being made. The knee gives way as the foot and shin are fixed but the momentum of the body continues over the knee.
A pop or snap is felt in the knee with severe pain. The knee often takes on an extreme position at the time of the injury. This usually corrects spontaneously. Typically the patient is unable to continue playing. The knee swells soon after. The knee continues to ache and feels unstable under foot.
An ominous sign is lack of swelling in the knee and marked pain and bruising on the inside of the calf indicating major ligament disruption. It is difficult to weight bear initially but as time goes on and pain subsides walking becomes possible and the knee settles down. As time goes the patient often feels the knee is unstable if they return to twisting type activities.
Treatment
The goal of treatment of an injured knee is to return to normal activities and prevent further damage to the important structures within the knee, the articular cartilage (gliding surfaces of the knee) and the meniscal cartilages (the shock absorbers of the knee). If the patient’s knee continues to give way and be unstable then further damage will occur to the articular cartilage and menisci leading to early onset osteoarthritis (wear and tear arthritis).
Treatment may be operative or non-operative. This often depends on the level of activity the patient wishes to pursue. The knee may become stable through a course of physiotherapy aimed at using the muscles about the knee to stabilise the knee. If the patient wishes to return to a high level of twisting type activities such as competitive ball sports or contact sports or skiing then surgery may become necessary.
The longer the knee is without an ACL and is unstable the more damage will occur and the worse the outcome will be. It can be argued that young patientswith active lifestyles or manual work loads that early ACL reconstruction may be beneficial. It is clear that very young patients, adolescents and teenagers should have their ACL reconstruction performed early to prevent further damage to the knee from instability.
If there is internal derangement to the knee such as a meniscal tear which needs repair or other ligamentous injury requiring repair then an early reconstruction is usually necessary. Surgical repair (a Knee Reconstruction) is a serious undertaking with a long rehabilitation programme. Typically it takes 6-9 months before a return to sport can be anticipated.
Download